

Continued from the introduction, this is a form of toxicity or intolerance that affects the central nervous system including the spinal cord and the brain. In extreme cases it can lead to grand mal (generalized tonic-clonic seizure) like convulsions, and unconsciousness. These have no lasting effect and cause no lasting damage with no sequelae and are harmless to the patient and are completely reversible and cessation is achieved by halting oxygen breathing. Remember the air breaks? One of the reasons we give divers or HBOT patients air breaks, is to avoid this side effect entirely.
US Navy and Royal Navy studies show that the air break almost eliminates the considerably minor risk when breathing pure oxygen under increased pressure. The only problem that may present is if the seizure causes the patient to injure or harm themselves by colliding with the hull of the chamber or other immovable object. Other than that, it causes no other harm and is extremely rare with incidents limited to exceptional exposure levels which we avoid.
With divers using bite mouthpieces, it can be more dangerous. The diver would spit the mouthpiece out and the consequences are obvious. This is one of the reasons commercial and military divers make use of full face masks or enclosed helmets which cannot easily come off. In a chamber environment there is no water. Problem solved. In any event, an attendant would be present in the chamber to manage any extremely unlikely occurrence. In the millions of exposures in the UK in the past 30 years at type 3 HBOT units, there are no recorded incidents.
We simply don’t go anywhere near the tolerable limit.

Notwithstanding that, and as mentioned in the previous introduction, this one is targeted at the scientists and medical professionals among us. for this reason we elaborate further for those with an interest in the science behind it all. This is not ordinarily information that a patient might receive routinely. It’s interesting though, even if just as an overview.

The measurement for CNS Toxicity is called the oxygen clock and is expressed in percentage. 100% being the most one can theoretically tolerate before seizure may become a real risk. That said, many a dry and wet dive has been conducted way beyond these limits with no occurrence of seizure. As little as 1 in 157,930 incidences are reported to result in seizure as indicated in studies undertaken by special ops diving units in the paper indicated in the graphic below. In other words, it’s a rare occurrence even under stress induced situations such as special forces diving. It’s even rarer and virtually unheard of in HBOT chambers. (Oxygen Toxicity and Special Forces Operations Diving Wingelaar Et al 2017)

This is a very well authored and referenced paper going into detail on the physiological causes of toxicity and is well worth a read. It describes mechanisms in more detail than can be presented here for the purposes of this article though. Not forgetting the reference in the introduction to this series which relates to hypoglycemic events on the other side of the blood brain barrier being a cause of seizure. Modern research is beginning to overturn previously held positions. It is however far more detailed than can be covered in this discussion. What it does establish though is that cerebral or CNS toxicity is not quite as common as previously thought and certainly not as easily induced as many would have you believe. I’ve heard of cases where people deliberately push the limit and fail to make it happen entirely. It also establishes that what may induce seizure on one day in a given subject, may not the next day. The variables for personal susceptibility are so varied that it is very difficult to apply a universal standard to the general population. There is no absolute value for this. Accordingly, the diving industry, including recreational, technical, commercial and military, have introduced “in-water” limits to be observed. They are considered to be well within the safety margins provided by the original US Navy and Royal Navy predictions. Varying organisations have slightly differing limits, but all follow in the same vein.
The oxygen clock is calculated by observing the partial pressure of oxygen being breathed and the time it is breathed for.
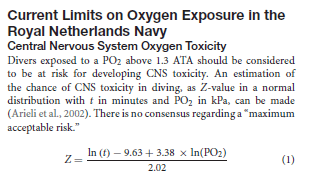
The Royal Netherlands Navy follows the following calculations for CNS exposure to oxygen. Incidentally, the equation can be extended to VO2 and variable metabolic rates as well. It’s not strictly necessary to understand the equation though. This is presented for the science enthusiasts among us. Most of us just use a pre calculated table of exposure when dealing with “in-water” applications. (Model of CNS O2 toxicity in complex dives with varied metabolic rates and inspired CO2 levels – Arieli R Israel Naval Institute – June 2003)
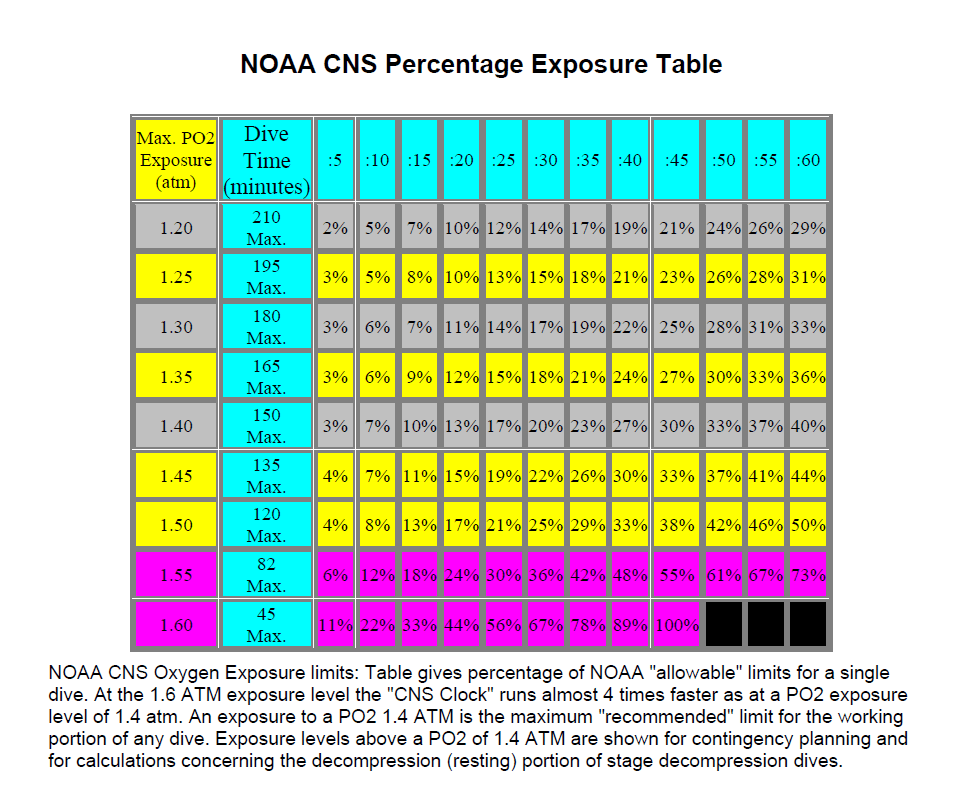
It must be stressed though that these limits are for “IN-WATER” application only. Because of the unique risk of drowning, the in-water limits are conservative to say the least, along with other contributing susceptibility factors present in water as previously mentioned. Many divers report exceeding these limits, by a huge margin, with no ill effect. No water in the chamber = no problem. It is ill advised to exceed the limits laid out below in the National Oceanographic and Atmospheric Administration (NOAA) table for in-water application.
Unfortunately uninformed individuals seem to advocate following in-water limits out of the water which is unnecessary. This unnecessarily limits the use of oxygen to the patients detriment.
These limits do not apply to the safe warm and dry environment of a hyperbaric chamber.
Commercial divers will observe slightly less conservative limits although not distant from the above table. Most recreational agencies have, these days, reduced their upper limit to 1,4 atmospheres absolute (ata), which is only just above the threshold at which seizure becomes possible (1,3ata), according to the USN diving manual as well as Royal Netherlands navy documentation, rendering exposure to higher partial pressures of oxygen (ppO2) relatively safe when following guidelines. For more on partial pressure refer to the article FLYING AND DIVING – A SOJOURN INTO PHYSICS AND PHYSIOLOGY.
To illustrate the difference between genuine exceptional exposure and what is often misrepresented as extreme exposure (HBOT), the following example is included:
Exceptional exposure air diving tables in revision 7 of the USN diving manual still allow for dives to a depth of 300 feet or approximately 92 meters on air. The “Exceptional Exposure” part of the title refers to both the nitrogen and the oxygen exposure. For the purposes of this comparison it is the oxygen exposure we refer to. At 92 meters of sea water the ambient pressure is a staggering 10,2 ata, or 10 times that of atmospheric pressure. While the body is quite OK at this depth, it is indeed an extreme exposure in terms of oxygen partial pressures. (United States Navy Diving Manual – 2016)
Breathing air at this depth equates to a partial pressure for oxygen of 2,14 ata. Certainly above any in-water limit discussed. A single exposure limit of 2,5ATA is allowable in US Navy procedures in exceptional circumstances. The usual in-water diving limit imposed by recreational, technical and commercial operators is 50 meters on air. For short exposures of up to 45 minutes the oxygen pressure is tolerable. At 50 meters the ambient pressure is 6ata and this equates to an oxygen pressure of 1,26ata. Well within limits. In fact, as far as oxygen goes it is relatively safe to spend 45 minutes at 66 meters breathing air. The ambient pressure being 7.6ata, breathing air equates to an oxygen pressure of just under 1.6ATA. The reason no one does this routinely is the because of nitrogen considerations including both the decompression penalty (the need to complete decompression stops on the way up), and something called nitrogen narcosis, a topic for another discussion. The deep air limit is very much a nitrogen-based limit and not strictly an oxygen consideration. Once an understanding of in-water limits is achieved, it makes it possible to draw a comparison between that and the comparatively benign and safe, chamber “diving” conducted at much lower pressures than those used in the example above. Routinely, and even in the case of diver re-compression, chambers are almost never compressed beyond the equivalent of 18 meters or 2,8 ata. This comparison illustrates that HBOT delivered in a chamber is nothing like the exposures and considerations involved in diving. It’s a different ball game entirely and the risk has been overstated by a great many.
This is further evidence that cerebral toxicity isn’t the unmanageable monster it is portrayed to be in mainstream medicine. Often the case may be that when an individual approaches a doctor to ask about hyperbaric oxygen therapy, the doctor may not have heard of it before or know much about it. This doesn’t mean there’s anything wrong with the doctor, but rather that they simply haven’t come across it before since it’s not routinely taught in universities save for specialist modules. When this happens doctors tend to fall back on the old position of toxicity and unfortunately they can discourage it’s use, and since people trust their doctors entirely, this is as far as it goes and the patient looses out on at least some relief and benefit from whatever their issue may be.
Certainly, exposures of 2.0 to 2.4 ata in a dry environment are comfortably tolerable by humans and easily managed with no lasting consequence in the event a person or patient does experience minor symptoms of intolerance. Varying susceptibility factors do come into it though, and lower tolerance limits are observed in individuals with intra cerebral issues as well as those who are particularly unfit among many other factors. This is however easily managed by simply giving them a break – an air break. (United States Navy Diving Manual Volume 5 3-9.2.2.4 – 2016).
Remember also that as operators or diving and hyperbaric supervisors, we are trained to spot any signs of trouble a mile off. An individual in the hands of an experienced and well trained diver is in good hands indeed. If it were me being treated, I would choose a diver over almost anyone else to drive the chamber.
Mention must be made of infants in closing, specifically prematurely born infants who receive HBOT. Infants are reportedly more susceptible to toxicity than adults and ocular toxicity has been noted in some cases. For this reason, dosage and duration of treatment is often modified to mitigate the additional risk and susceptibility. This should not be construed as a contra indication but rather cause to monitor or modify protocols at most. Even newborns can be treated in free flow boxes and modified hood and this shouldn’t be a cause to avoid treatment entirely.
For the above reasons, we dismiss in-water limits in HBOT as we will most certainly exceed them all and they DO NOT APPLY anyway. Since we aren’t in the water and no water is involved, why would we adopt water related limits? It would be like driving at 20 mph on the motorway for no good reason.
We do however observe the recommended upper limit of 2,8 ATA, and generally speaking, re-compression or HBOT treatments do not exceed this for any significant duration. With only rare case studies reaching as high as 4 ata for brief periods but it is definitely not the norm. In fact, most HBOT protocols are well inside this limit and generally a dosage pressure of 2ata to 2,4 ata is observed for periods not normally exceeding 90 minutes. Mostly there is little established significant additional benefit above these pressures and times.
The volunteer managed, and de-regulated type 3 HBOT chambers in the UK generally do not exceed 2 ATA, with many favouring 1,75 ata as their preferred protocol pressure for optimal neurological benefit. Additionally, if the therapy pressure calls for it, and not all of them do, air breaks, commonly accepted as standard, further protect against CNS O2 Toxicity and intolerance and prevent any side effects.
Air breaks extend protection beyond CNS toxicity as well. They help protect the lungs from the other main form of toxicity, Pulmonary Toxicity.
In part three we will conclude with a discussion on pulmonary toxicity and matters relating to how long term repetitive exposure to oxygen affects the lungs. We will also introduce readers to the Repex Method of tracking whole body toxicity through the tracking of Oxygen Tolerance Units or OTU’s.
©Hayden Dunstan

Is the NOAA percentage table for air pressure only (21% O2) or pressure + 100% oxygen?
LikeLike
Hi Tony. The NOAA table shown in the article tabulates exposure limits for central nervous system (CNS) toxicity only. It is based on the partial pressure of oxygen (pp02 or sometimes called p02) exposed to and the duration of exposure. Partial pressure of oxygen can be calculated using the oxygen percentage of the mix all the way from zero up to 100%, and pressure in atmospheres. For example: for air at 21% oxygen the partial pressure of the oxygen at sea level or 1 atmosphere (ata) would be 0,21 ata pp02. For 100% oxygen at sea level of 1 ata it would be 1 ata. This is arrived at by multiplying the pressure by the percentage expressed as decimal fraction. air (21% oxygen) is expressed as 0,21 pp02 at 1ata. therefore at 2 ata or 10 meters depth it would be twice that, arrived at by multiplying the percentage expressed as a decimal by the pressure: EG: 0,21 ata pp02 X 2 ata = 0,42 ata pp02. The table isn’t specifically for air or any specific pressure or depth it is for partial pressure which comes from calculating percentage against pressure represented as a fraction of the total ambient pressure. Remember though that cerebral or CNS limits are entirely for in water or “wet” application. They do not apply in a dry chamber. The article includes this information as background information which helps to better understand where whole body toxicity and the concept of oxygen tolerance units (OTU’s) come from. Almost every chamber treatment protocol will exceed these diving CNS limits so we don’t usually use at that table. The table was originally researched and designed for divers actually in the water who’s physiology responds differently to a dry chamber. For this reason occupants of a chamber needn’t worry about the diving limits for CNS exposure since their physiology is behaving significantly differently being dry, warm and at rest. We tend to use whole body toxicity in hyperbaric chamber work which you can read more about in part three of the 3 part series. Part 2 explains pulmonary toxicity being longer term exposure of the lungs to high concentrations of oxygen. I hope this helps. Please let me know if you ned any further help. Regards , Hayden.
LikeLike