
It may seem a little clumsy to group these conditions under a single heading as they differ greatly in many ways in their onset, direct causes and individual pathologies. However, as far as HBOT and complementary therapy goes, specifically oxygen therapy, they share one commonality among them, hypoxia (low oxygen, or lack of oxygen). In all of these neurological conditions it’s the underlying hypoxia, that according to a quote by John Scott Haldane, Scottish physiologist and the father of oxygen and diving theory, is the mechanism that is responsible for physiological deficit. He said:
“Hypoxia not only stops the machine, it wrecks the machinery.”
In all cases, as we have previously discussed, wound healing principals apply in both the micro, (small), and the macro, (large). Essentially we target the cause of the perpetuation of an injury whether that injury is a microscopic injury in the brain, or a macroscopic wound on a foot or leg. We target the underlying hypoxia that causes it to become problematic by giving more oxygen. And whats more, we give more oxygen than ordinary oxygen therapy can deliver to tissue. We give exponentially more by increasing the pressure and consequentially the plasma load. This not only acts as a therapy after an event, hopefully reversing ischaemia and repairing damage, but also as a prophylaxis and protective agent which helps prevent incidents in those with a higher likelihood of occurrence and those with higher risk factors such as permanently narrowed arterial structures and other arterial insufficiency. As supported by the Undersea and Hyperbaric Medical Society (UHMS). Such arterial insufficiency can lead to stroke and other neurological and ocular complications.

For regular readers, at this point, the mechanisms of cell repair and rebuild, and the motivation behind the belief and support of wider spread HBOT commissioning begins to become somewhat repetitive. Many of the mechanisms and physiological functions attributed to wound healing, anti-inflammatory response, mild traumatic brain injury, improved glycolysis, improved glycogenesis and gluconeogenesis and so on, are shared by multiple conditions. In fact I was pleased with a recent confirmation that cellular metabolism is biological life itself. At the cellular level it is the primary driver of all things including the natural healing envelope. HBOT simply extends that envelope. It’s the body that does the healing.
In a very apt video clip from Ocala Health Florida, their Cameron Baldwin discusses fatigue. Mr Baldwin comments, “It’s like running a race in there”. And this is from his personal observation. Well done for stating it so unequivocally. Improved metabolism as a result of HBOT is indeed like having a workout. We simply don’t feel it the same way we do when we actually work out since cellular function at this level is not connected to the sympathetic nervous system. Then of course, sleep follows as we discussed in the article SLEEP – THE ELIXIR OF LIFE.
Optimal oxidative cell metabolism, (which is based on oxygen availability and use), facilitates cell growth, division, and tissue repair. It allows for optimised angiogenesis, (new blood vessel growth) and tissue development following injury or illness. This is familiar to all tissue systems, organs and other biological systems.
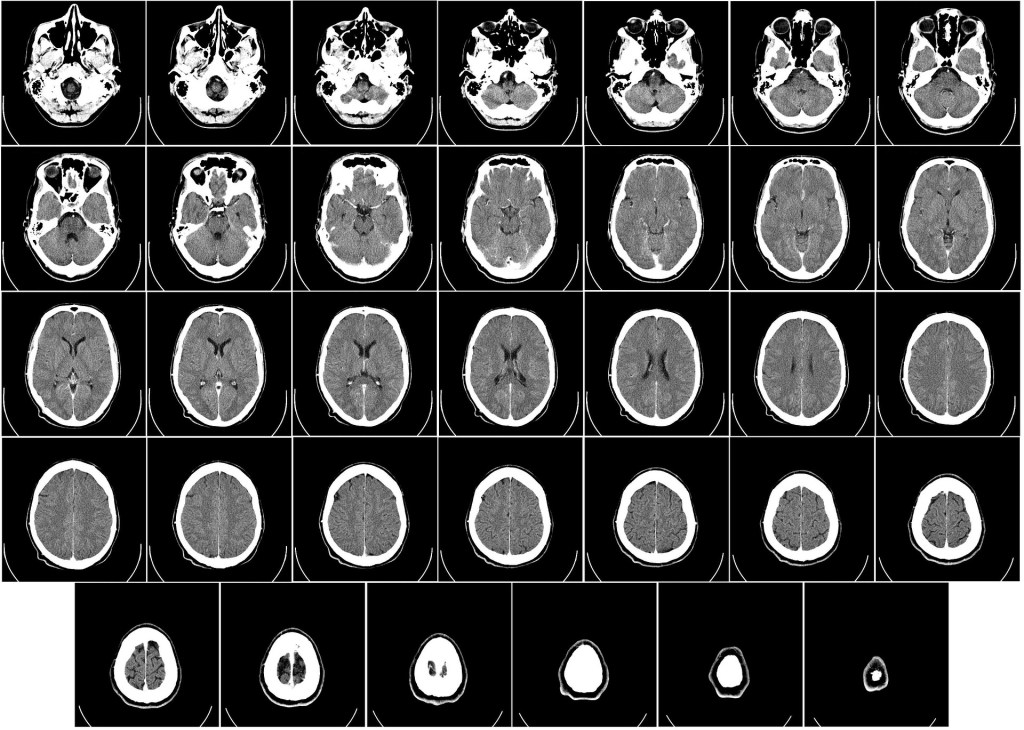
Injury in the brain, following stroke for example, really only differs in that brain tissue, once truly lost doesn’t regrow in the same way other tissues grow, if it regrows at all. There are however those cases where brain tissue is not completely lost but rather rendered ischaemic following a hypoxic episode. And that really is all it is, an hypoxic episode caused by a blockage or other vascular failing. This is the tissue that can potentially be rejuvenated by improving oxygen transport to those cells affected. Granted, HBOT won’t necessarily benefit ALL stroke patients since we can’t know to what extent tissue is necrotic or ischaemic. In cases of stroke, patients often report loss of eyesight on one side or the other. This too can result from ischaemia and doesn’t necessarily indicate necrotic cells and tissue. SPECT imaging can show up areas of necrotic tissue and those areas which are ischaemic by highlighting blood flow in the brain. Please note that necrotic tissue cannot be rejuvenated. Oxygen can only act on cells which haven’t yet become necrotic. Salvaging ischaemic tissue in conjunction with newly established evidence of continued nueroplasticity throughout life gives cause for hope. By salvaging what is possible to savage, in conjunction with other therapies, brain function, through continued plasticity, can potentially develop new pathways through which to function.
Very recent research claiming that neurons continue growing throughout the life of a human with perhaps a finite number of mother cells for life but a continued growth of daughter cells, which then divide and differentiate into becoming neurons, gives additional cause for hope. (Boldrini Et al 2018)
Brain tissue is far more sensitive to a state of hypoxia. Brain or central nervous system injury can lead to irreparable damage which can be minimised when early intervention is implemented. It can also be relieved to some degree where ischaemic tissue is considered. Some brain function may seem lost, and the prevailing conclusion is irreparable brain damage. However, this may be due to ischemic tissue not functioning as intended. This tissue can be recovered as it is not yet necrotic. Ischemic tissue can perpetuate for years and still be rejuvenated as researched by Prof Shai Efrati of the SAGOL Hyperbaric Medicine Unit at the Shamir Medical Center in Tel Aviv. This is witnessed by at least some improvement in patients even some years following neurological insult. Even well down the line in the case of dementia patients as well as some motor degenerative patients as is the case in Parkinson’s Disease. Subjective as they may be, testimonials abound as to the improved quality of life for these patients.
In vascular dementia or stroke resulting from cerebral vascular disease, brain cells die or become ischaemic following vascular compromise in the brain. Similarly, post traumatic dementia follows injury in the brain leading to cell death or ischaemia. Incidentally it is also speculated that head injury can lead to Parkinson’s Disease with cell death and ischaemia in the substantia nigra, a region of the mid brain. Its the ischemic cells that can potentially be salvaged.
What if we could catch and save some of those cells not quite gone yet? Surely even symptomatic relief is something? In Lewy body dementia as well as Alzheimer’s disease and Parkinson’s disease, clumps of protein (Lewy Bodies), have been found in the brains of patients. This is one of the more common types of progressive dementia. Owing to the vasoconstriction HBOT induces, it is reasonable to assume that an optimally functioning and protected blood/brain barrier, would keep these bodies out of the brain where they don’t belong. There are many types of neuro-degenerative disease which can fall under the umbrella of dementia. Too many to detail here. They all have one thing in common though. Hypoxia induced brain dysfunction.
All of these conditions grouped under dementia seem to share a commonality. Compromised vascularisation. Indicating that cerebral dysfunction of this nature could indeed be a vascular condition allowing debris and emboli into the brain through a compromised blood brain barrier resulting in microscopic injury. HBOT is known to protect the blood/brain barrier by means of vasoconstriction which renders capillaries less permeable. Explained previously, an increase in oxygen tension can and does enable adequate oxygenation of tissues including brain tissue. It’s a workaround when vascularisation is compromised. HBOT also helps restore vascularisation as it up-regulates angiogenesis. This most certainly would be of benefit where sensitive brain tissue is concerned.
Perhaps not a cure, but certainly an ongoing management tool for improved quality of life. Many patients undergo therapy reporting good results. Memory and cognitive function seem to benefit to some degree and quality of life is better. Stroke patients report regaining at least some function and degenerative disorders alleviate, providing relief to family’s and patients alike.
Unfortunately, mentioned before, this is not a cure, no one is claiming it is. It is a therapy though, and that is fortunate indeed.
That’s why it is called “Hyperbaric Oxygen Therapy” and not “Hyperbaric Oxygen Cure”. While it can cure some things outright, it can also be used a complementary and adjunct therapy in many other cases such as these.
As a result, in some conditions, therapy is best when continued indefinitely. Cognitive dysfunction will likely continue to relapse if therapy ceases altogether. Reports however, claim that following an initial series of “treatments”, less frequent maintenance sessions are sufficient to maintain ongoing good outcomes and positive results.
This has lead to the development of Mild Hyperbaric Oxygen Therapy (mHBOT). These are soft shelled chambers for home use. They are safe and easy to use. Pressure does not exceed 1,4ATA. They are reasonably affordable although still not cheap. They are becoming more common and have potential as ongoing therapy following initial treatments. This is discussed in the article DOSAGE: HBOT AND MHBOT.
As discussed in the physics articles, fast tissues, (Haldane again), benefit from relatively low pressures, which allows for extended duration of exposure. mHBOT soft chambers could prove ideal for neuro degenerative disorders since the brain is a relatively fast tissue and saturates relatively quickly compared with say, bone. They can be put in the corner of your room and used once or even twice a day. Many testimonials are available on the internet as to the success enjoyed by many. Unfortunately, there are some that take advantage of this. Some private units tend to charge an awful lot for treatment, making it inaccessible to many. Given also that mHBOT delivers a much lower dose than a full size hard shelled chamber adds insult to this. Healthcare for the rich syndrome and profiteering. The motivation for government funded healthcare to include HBOT for wider application must be ongoing to make this modality a mainstream and routine modality.
One in every medical center would do.
©Hayden Dunstan
